Results of the Research Equity, Diversity and Inclusion Demographic Survey
In late 2019, Unity Health Toronto’s Research and Innovation enterprise signed on to the Dimensions Charter, pledging to join more than 50 academic research institutes in an initiative started by the Government of Canada to drive deep cultural change in the research ecosystem in Canada. The charter’s focus is on eliminating obstacles experienced by members of underrepresented or disadvantaged groups, including, but not limited to, women, Indigenous Peoples, persons with disabilities, members of racialized groups, and members of LGBTQ2+ communities.
As part of this commitment to equity, diversity and inclusion (EDI), Research leadership created a baseline demographic survey to measure and improve EDI strategies in our workplace. The survey was modelled after the University of Toronto Employment Equity Survey. The response was overwhelming – nearly 60 per cent of our community participated in the survey. The response rate amongst scientists was 64 per cent, amongst trainees it was 60 per cent, amongst research and support staff, it was 51 per cent.
Highlights of the survey results are outlined below.
What will we do with this information?
Our baseline data will inform future strategies and help us measure our progress. These strategies will build on our ongoing practice which has included:
What did the survey show us?
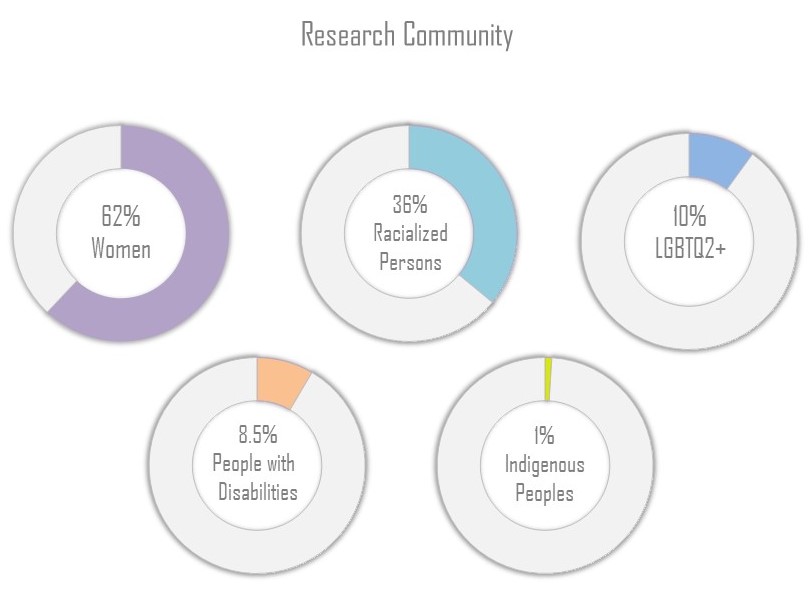
First, we found out that the majority of our research community are women (62%).
Thirty-six per cent identify as racialized. Members of racialized communities in Canada are persons, other than Indigenous Peoples, who are non-Caucasian in race or non-white in colour, regardless of place of birth or citizenship. The responses to the question in the survey about race and ethnicity are further analyzed in the graphs that follow.
Further, about 10% of our community identifies as LGBTQ2+, which in the purposes of this survey were defined as gay, lesbian, bisexual, transgender, queer, two-spirit or other.
Our survey also showed that 8.5% of respondents self-identified as a person with a disability. Based on the definitions from the Federal Contractors Program, “persons with disabilities” are persons who have a long-term or recurring physical, mental, sensory, psychiatric or learning impairment(s) AND who consider themselves to be disadvantaged in employment by reason of that impairment, OR believe that an employer or potential employer is likely to consider them to be disadvantaged in employment by reason of that impairment.
One per cent of respondents self-identified as an indigenous person. An “Indigenous person” could be First Nations (status, non-status, treaty or non-treaty), Métis, Inuit, Native American, Alaska Native, or Native Hawaiian.
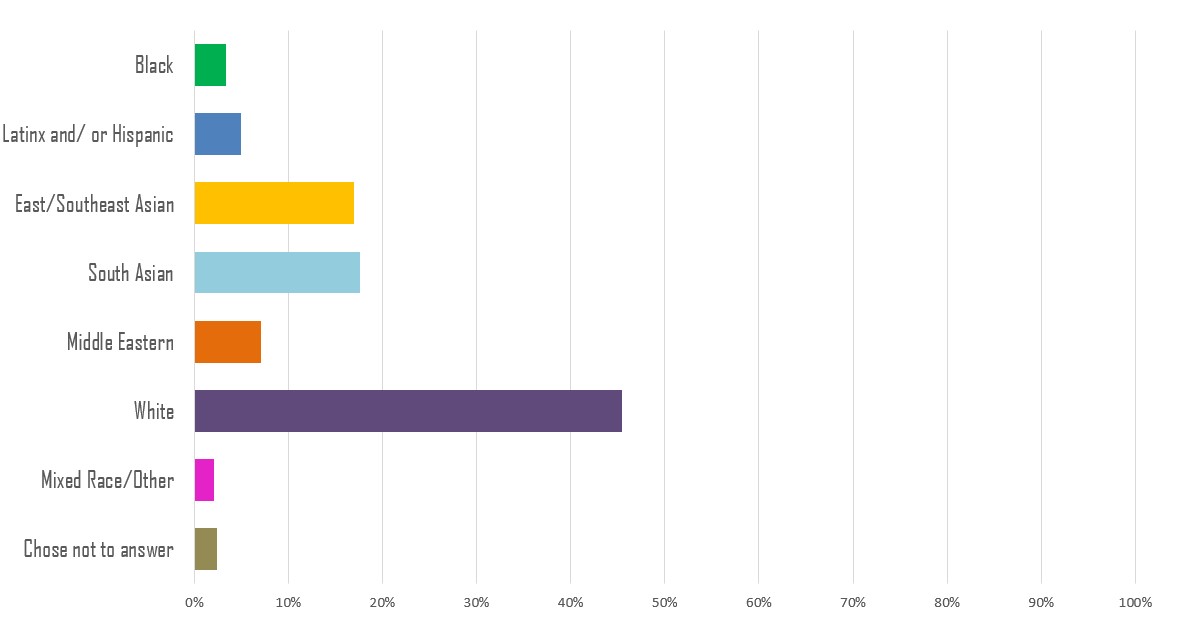
Of those who identified as racialized, most identified as South Asian (18%), East/Southeast Asian (17%), and Middle Eastern (7%). Other groups included Latinx or Hispanic (5%), Black (3%) and Mixed Race/Other (2%).
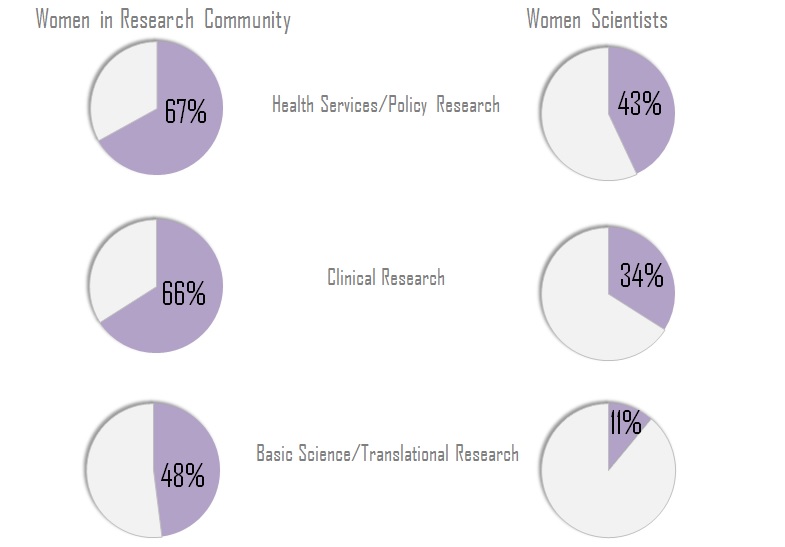
Out of those who identified as women in Research, the majority (67%) work in Health Services and Policy Research. In Clinical Research, 66% are women, and 48% in Basic/Translational Science are women.
Forty-three per cent of scientist respondents in Health Services/Policy Research identified as women, along with 34% in Clinical Research and 11% in Basic/Translational Research.
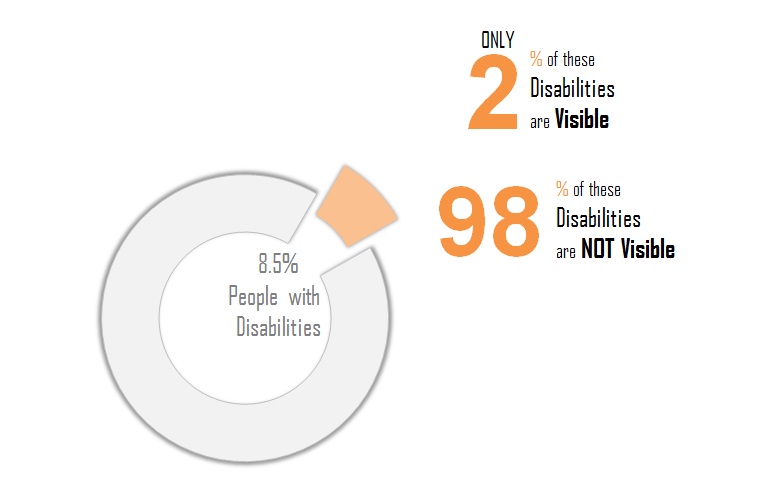
Of the respondents in the research community, 8.5% said they have a disability, only 2% of which are visible disabilities. The rest are non-visible, or “invisible,” both of which are terms commonly used to describe a disability that is non-evident or not readily apparent to others.
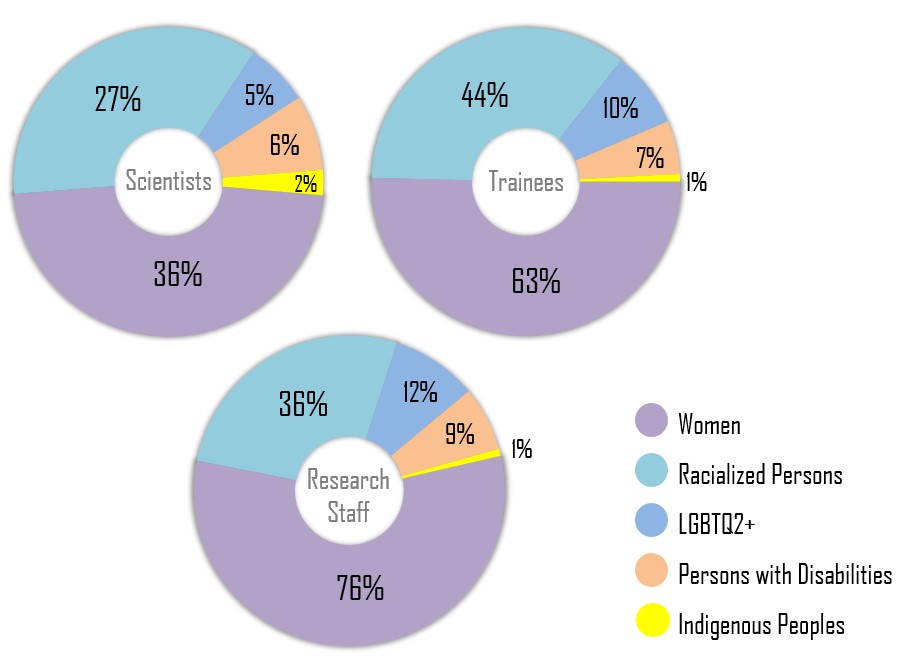
When analyzing by role, the survey suggested that 36% of scientists are women, 27% identify as racialized, 6% are persons with disabilities, 5% identify as LGBTQ2+ and 2% are Indigenous Peoples.
Amongst trainees, 63% are women, 44% are identify as racialized, 10% identify as LGBTQ2+, 7% are persons with disabilities and 1% are Indigenous.
And, amongst Research staff, the survey found that 76% are women, 36% are racialized persons, 12% are LGBTQ2+, 9% are persons with disabilities and 1% are Indigenous peoples.
What’s next?
With this information, we aim to create strategies that promote equity, diversity and inclusion in Research and Innovation at Unity Health. To that end, we’re developing and exploring faculty development and educational materials on EDI. We will also be expanding our gender equity search committee guidelines in Research to include other equity priorities in addition to gender.
Unity Health’s Research leaders are also participating in a Toronto Academic Health Sciences Network-Research (TAHSN-R) wide working group with an intent to share information and identify best practices to create a more equitable, diverse, and inclusive research environment across TAHSN institutions. The Working Group will identify priority actions and determine next steps that will allow the University and the affiliated hospitals to work collaboratively to develop and implement these practices.
We also want this data and information to contribute to a fulsome strategy at Unity Health. We have started working with the Education and Human Resources departments to support and inform a network approach to EDI that will ensure multiple engagement strategies.
We know research and innovation is more impactful when its community is representative of the population our hospital and our knowledge serves. Like any good research, our work starts with data. We aim to conduct this survey on a regular basis to measure whether we have moved the needle and to gain valuable feedback from our community that will guide our future EDI work.
To review the questions that were posed in the survey, please see the PDF version of the survey here.
If you have questions related to EDI in research, please contact VPRI@smh.ca.