The burdens of out-of-hospital cardiac arrest and life-threatening traumatic injury are, at best, only crudely known. Whether and how EMS process, geographic, socioeconomic and periodic variation are associated with differences in outcome is unknown. This can be largely attributed to the absence of any internationally-representative epidemiologic database that includes outcome. Knowledge of factors related to specific episodes, together with regional factors including EMS system factors and outcome is a first step toward the development, implementation and evaluation of interventions to improve outcomes associated with these illnesses.
Specific aims of the Epistry registry are to:
How are these goals met?
Epistry works on the basis of moving data from front line responders to the registry where it can be analyzed by members of the research team. This involves a group effort to collect and interpret data from patient charts, defibrillators, dispatch centres and more. The types of information collected varies based on patient, but ranges from demographics (such as age, gender and location), interventions (such as CPR, medications, and surgeries), and outcomes (such as survival and neurological functioning).
In order to meet these goals, patient identifiers are used to make sure patients can be appropriately followed up through their course of care and linked to provincial datasets where appropriate. All patients are de-identified for analysis and their identities are never disclosed. Aggregate data is then used to assist in local agencies and institutions in improving patient care, and in the publication of scientific papers to share our findings with the worldwide resuscitation community.
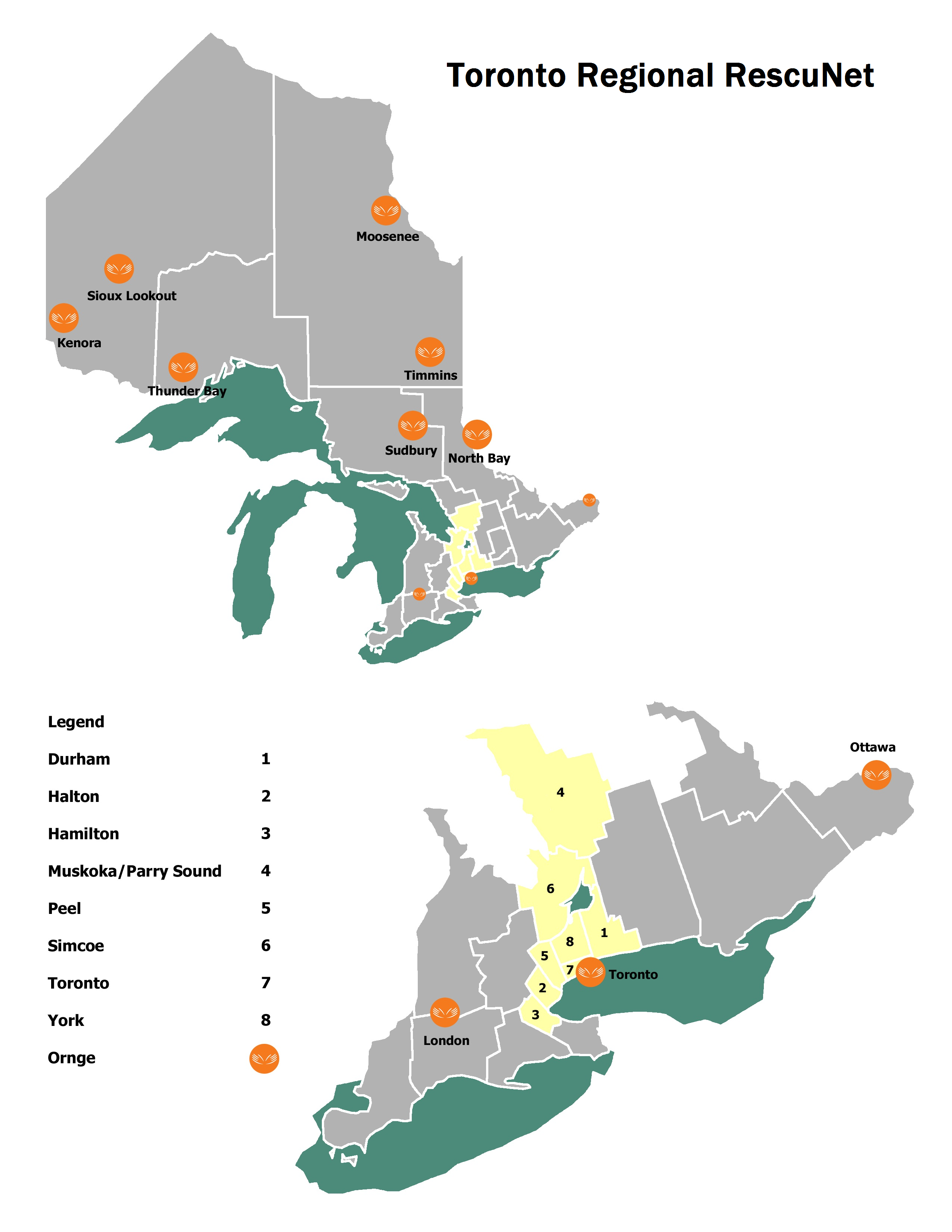
The Toronto group has been renamed the Toronto Regional RescuNet for Toronto Regional Resuscitation Research Network. Collaboration of these regions provides a large urban and rural patient population in close proximity to each other to conduct randomized control trials.